Авторы: Jerome A. Dempsey , Peter D. Wagner 2006 год
*Краткое содержание от переводчика — у спортивных, тренированных людей зачастую наблюдается артериальная гипоксимия, т.е. сниженное кол-во кислорода в артериальной крови. Это снижает способность мышц потреблять кислород. Механизмы которые всем этим управляют до конца не ясны, но организм может резко ограничивать потребления кислорода мышцами. Возможно проблема в обьеме лёгких, и те кто имеет больший их объем имеют преимущество. Если тема интересна и хотите перевод — жмите лайки!
Exercise-induced arterial hypoxemia (EIAH) at or near sea level is now recognized to occur in a significant number of fit, healthy subjects of both genders and of varying ages. Our review aims to define EIAH and to critically analyze what we currently understand, and do not understand, about its underlying mechanisms and its consequences to exercise performance. Based on the effects on maximal O2uptake of preventing EIAH, we suggest that mild EIAH be defined as an arterial O2saturation of 93–95% (or 3–4% <rest), moderate EIAH as 88–93%, and severe EIAH as <88%. Both an excessive alveolar-to-arterial PO2 difference (A-a DO 2) (>25–30 Torr) and inadequate compensatory hyperventilation (arterial PCO2 >35 Torr) commonly contribute to EIAH, as do acid- and temperature-induced shifts in O2 dissociation at any given arterial PO2 . In turn, expiratory flow limitation presents a significant mechanical constraint to exercise hyperpnea, whereas ventilation-perfusion ratio maldistribution and diffusion limitation contribute about equally to the excessiveA-a DO 2. Exactly how diffusion limitation is incurred or how ventilation-perfusion ratio becomes maldistributed with heavy exercise remains unknown and controversial. Hypotheses linked to extravascular lung water accumulation or inflammatory changes in the “silent” zone of the lung’s peripheral airways are in the early stages of exploration. Indirect evidence suggests that an inadequate hyperventilatory response is attributable to feedback inhibition triggered by mechanical constraints and/or reduced sensitivity to existing stimuli; but these mechanisms cannot be verified without a sensitive measure of central neural respiratory motor output. Finally, EIAH has detrimental effects on maximal O2 uptake, but we have not yet determined the cause or even precisely identified which organ system, involved directly or indirectly with O2 transport to muscle, is responsible for this limitation.
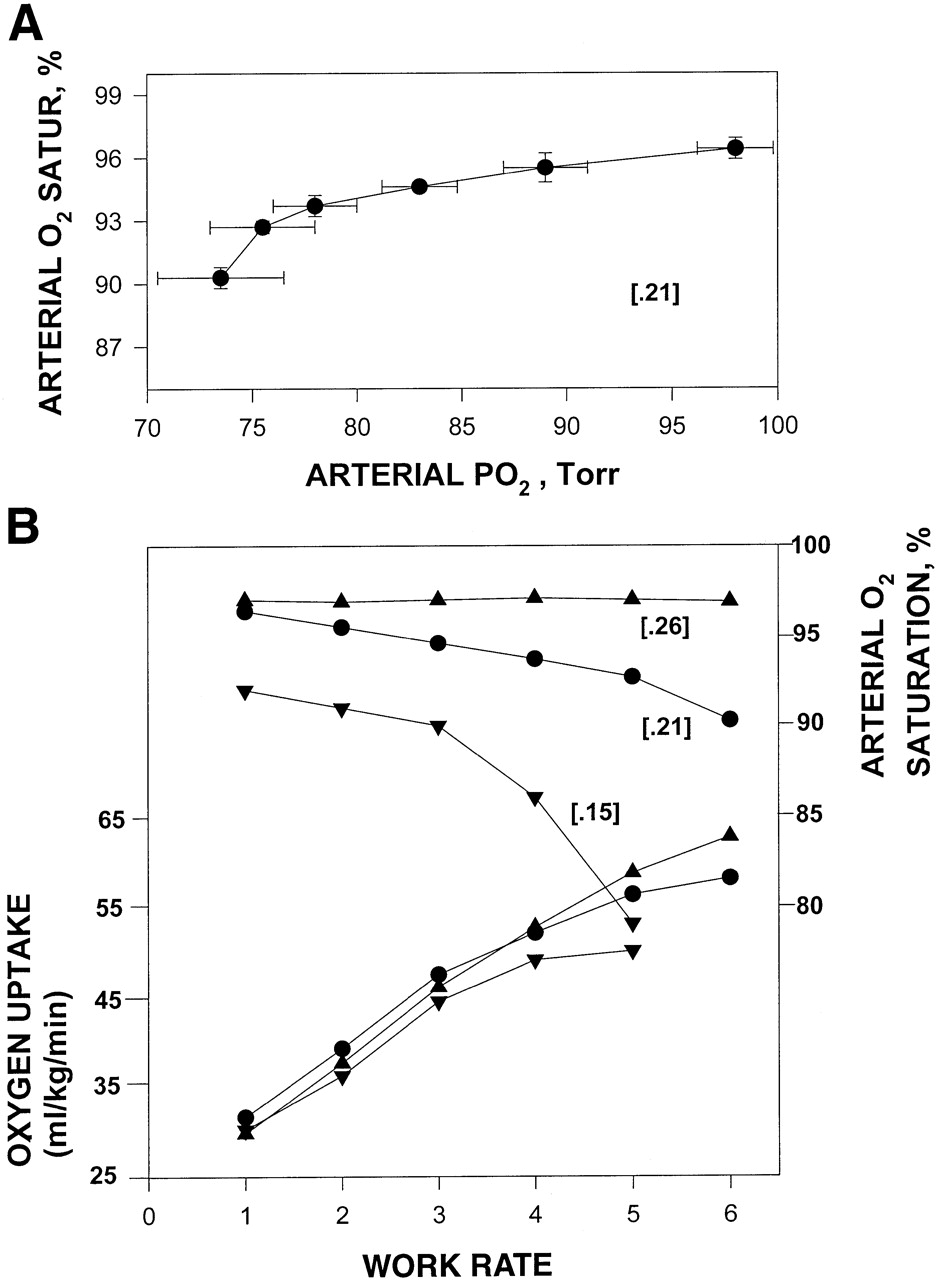
Exercise-induced arterial hypoxemia in fit humans (n = 15 young women) during treadmill running. “Work rates” refer to an increasing treadmill grade of 2% every 2.5 min while speed is maintained at 6–10 miles/h.A: exercise-induced arterial O2 desaturation at maximal exercise due almost equally to a reduction in  and a rightward shift in the HbO2 dissociation curve (acidic pH = 7.29; temperature = 38.2°C). Also, note reduction in
and a rightward shift in the HbO2 dissociation curve (acidic pH = 7.29; temperature = 38.2°C). Also, note reduction in  beginning at submaximal work rates and progressing to maximum. B: effect of preventing exercise-induced arterial hypoxemia (EIAH) (via
beginning at submaximal work rates and progressing to maximum. B: effect of preventing exercise-induced arterial hypoxemia (EIAH) (via  of 0.26) and of acute hypoxia (
of 0.26) and of acute hypoxia (  of 0.15) on
of 0.15) on  andV˙O 2. Note that changes in
andV˙O 2. Note that changes in  do not affectV˙O 2 at submaximal work rates but do change the plateau effect at and near peak work rates. The 0.21 and 0.26
do not affectV˙O 2 at submaximal work rates but do change the plateau effect at and near peak work rates. The 0.21 and 0.26 data are from Refs. 13 and 14, and effects of 0.15
data are from Refs. 13 and 14, and effects of 0.15  were estimated from data in Refs. 7 and 28.
were estimated from data in Refs. 7 and 28.
